Large Integral Scale of Low Prolactin Markers
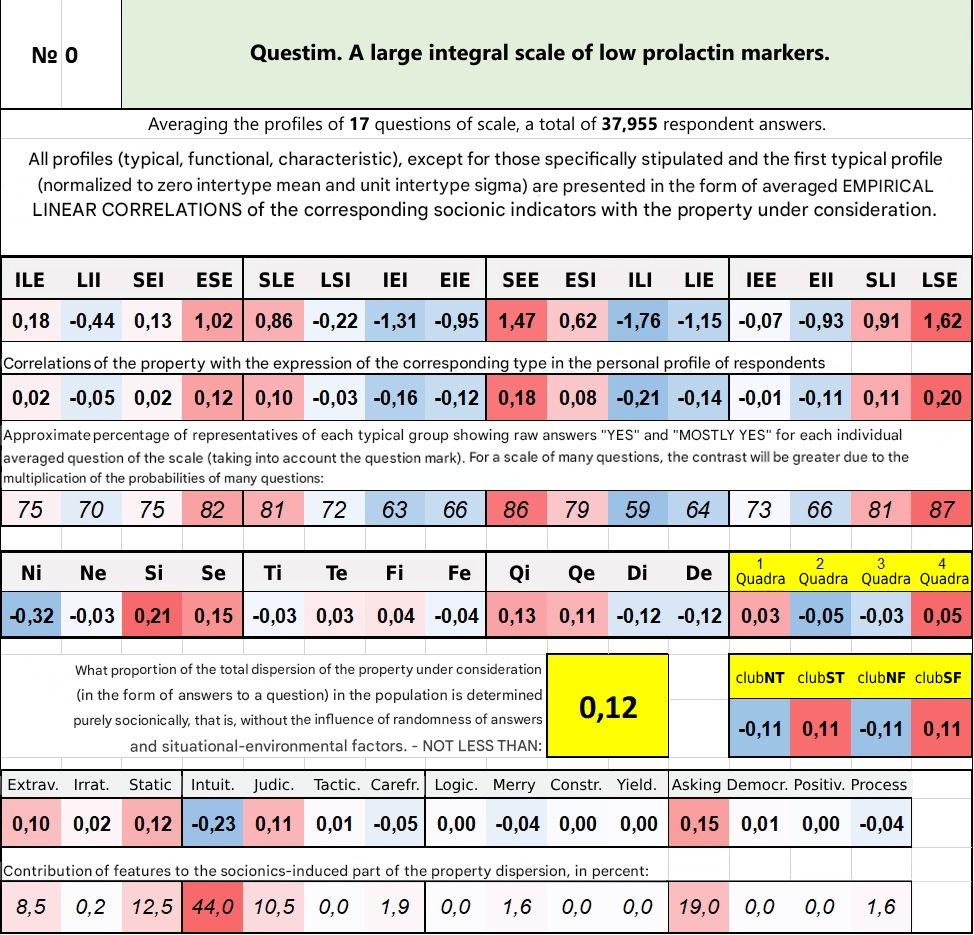
As we can see in the final table, the highest prolactin level (and simultaneously, the lowest dopamine – judging by the low activation of dopamine D2 receptors associated with high prolactin) is found in the ILI psychotype. Menstrual cycle disorders caused by elevated prolactin levels, resulting in delayed periods, are most commonly observed in women of the ILI, LII, and LIE types (especially frequently in ILI).
The synthesis and secretion of prolactin are directly stimulated by estrogens present in the blood. Therefore, the average level of prolactin in the blood of women (outside of pregnancy) is approximately one and a half times higher than in men. Dopamine, released in the hypothalamus, reduces prolactin levels.
In the last trimester of pregnancy, prolactin in a woman’s blood increases about 10 times more.
When a newborn is placed on the breast and starts sucking the nipple, it stimulates mechanoreceptors located on the nipple. The mechanoreceptors send a signal to the hypothalamus, initiating the milk ejection reflex. The stimulation of nipple mechanoreceptors is transmitted via afferent fibers through the spinal cord to the hypothalamus, which inhibits dopamine release, leading to increased prolactin concentration in the blood. During pregnancy, lactation does not begin despite high prolactin levels. This is because milk secretion is inhibited by the hormone progesterone, whose concentration drops after the placenta is delivered following childbirth, making lactation possible.
Prolactin production significantly increases during stress, anxiety, depression, severe pain (e.g., injuries, surgeries), and psychoses. Prolactin secretion increases even more during pregnancy and especially during lactation (breastfeeding). During pregnancy, estrogen levels increase, which leads to increased prolactin concentration. As a result, high prolactin levels cause the maturation and enlargement of mammary glands in preparation for lactation. Prolactin secretion also increases with alcohol and drug abuse (opiates, amphetamines, cocaine, cannabis), with the use of certain psychotropic drugs—especially antipsychotics, to a lesser extent antidepressants, tranquilizers, mood stabilizers—as well as with the intake of estrogens, contraceptive pills, and some antiemetics. Prolactin secretion decreases with dopamine D2 receptor agonists (bromocriptine, pergolide, cabergoline, and others), as well as with estrogen antagonists tamoxifen, clomiphene. To some extent, prolactin secretion decreases with thyroid hormones and glucocorticoids.
Prolactin is responsible for inhibiting the ovulatory cycle by suppressing the secretion of follicle-stimulating hormone (FSH) and gonadotropin-releasing hormone (GnRH). In women, prolactin prolongs the existence of the corpus luteum (lengthening the luteal phase), inhibits ovulation and new pregnancy, reduces estrogen secretion by ovarian follicles, and reduces progesterone secretion by the corpus luteum. Normally, this physiological mechanism prevents pregnancy with the next child during breastfeeding of the previous one and may suppress menstruation during breastfeeding.
Prolactin apparently has some analgesic effect. Reducing prolactin secretion with specific substances increases pain sensitivity in animal studies, while increased prolactin levels decrease pain sensitivity. It is assumed that one of the mechanisms (although not the main one) of the analgesic effect of opioid analgesics like morphine, as well as the nonspecific analgesic effect of antidepressants, antipsychotics, and tranquilizers, is the increased secretion of prolactin they cause. Apparently, the analgesic effect of prolactin is naturally intended so that nipple biting by the child does not cause excessive pain in the nursing mother. It is believed that prolactin is involved in endogenous opioid mechanisms of analgesia and the transformation of physical pain and mental humiliation into a pleasant state. This may explain the correlation shown in several studies between masochistic experiences and the feeling of "sweetness of one's guilt" with elevated prolactin levels in the blood.
Prolactin inhibits the action of dopamine, which is responsible for sexual arousal. Prolactin prolongs the refractory period after orgasm (premature ejaculation in men is often associated with excessively low prolactin levels in the blood).
It is hypothesized that prolactin is involved in immune responses. Its secretion by lymphocytes and other leukocytes increases with immune activation, inflammation, infections, and decreases with immunosuppression (treatment with immunosuppressants, glucocorticoids, anticancer chemotherapy). On the surface of many immune cells, there are prolactin receptors, and prolactin exerts an immunostimulatory effect on them.
Prolactin follows daily and ovulatory cycles. Normally, its peak level occurs during REM sleep and early in the morning. Many mammals experience a seasonal cycle. Physical exertion, eating, and sexual intercourse can cause increased prolactin levels.
During pregnancy, high circulating levels of estrogens and progesterone raise prolactin levels by 10–20 times. Estrogen and progesterone suppress prolactin’s stimulatory effect on milk production. A sharp drop in estrogen and progesterone levels after childbirth allows prolactin, whose level temporarily remains high, to induce lactation.
With hyperprolactinemia (outside of pregnancy), women experience menstrual cycle disruptions. Strong and sustained prolactin elevation can lead to infertility, anorgasmia, frigidity, decreased libido, enlargement of the mammary glands up to macromastia (giant breasts), cysts or adenomas of the mammary glands, and eventually even breast cancer. With a strong prolactin increase, galactorrhea is typical. Very high prolactin levels can cause mental illness. In men, chronic prolactin elevation may lead to decreased erections and reduced libido. In women, chronically elevated average prolactin also leads to decreased libido. Elevated prolactin in both men and women is associated with increased bone fragility due to decreased bone density and an increased risk of developing osteoporosis.
In music psychology, it is suggested that prolactin may play a role in the pleasurable perception of sad music, as prolactin levels rise when a person feels sad, exerting a comforting psychological effect. [1]
Prolactin rises after epileptic seizures [2] or due to physical or emotional stress. [3] [4] In a study on volunteers under hypnosis, prolactin release resulted from hypnotically induced humiliating experiences, while fantasizing about breastfeeding under hypnosis did not cause prolactin elevation. [4]
REFERENCES:
- Huron, David (July 13, 2011). "Why Sad Music Makes Us Happy? A Possible Role of Prolactin". Music Sciences. 15 (2): 146–158. doi:10.1177/1029864911401171. S2CID 45981792.
- Mellers JD (August 2005). "Approach to patients with 'nonepileptic seizures'." Postgraduate Medical Journal. 81 (958): 498–504. doi:10.1136/pgmj.2004.029785. PMC 1743326. PMID 16085740.
- "Prolactin". MedLine Plus.
- Sobrinho LG (2003). "Prolactin, psychological stress, and environment in humans: adaptation and maladaptation." Pituitary. 6(1): 35–9. doi:10.1023/A:1026229810876. PMID14674722. S2CID1335211.
INTEGRAL CLUSTER QUESTIONS FOR LOW PROLACTIN
AGREEMENT WITH ITEMS (low prolactin markers):
- It is true that I have no predisposition to swelling in the face or legs. 0.412
- I believe that compared to other people, my bones are strong and healthy – at any rate, I’ve never broken anything and haven’t complained about bone pain. 0.504
- I have a very easily excitable sexual desire. 0.268
- It is true that I have never had any allergic reactions in my life. 0.117
DISAGREEMENT WITH ITEMS (high prolactin markers):
- At times I am interested in painful and humiliating sensations, and feel a certain "high" while experiencing them. -0.931
- Sometimes it feels pleasant to experience submission and humiliation. -0.924
- My menstrual cycles are irregular – with delays and disruptions of a week or more (female). -0.687
- My skin, unfortunately, is prone to acne and pimples. As soon as some clear up, others break out. -0.652
- During sex, I often can’t "finish" (no approach of orgasm, ejaculation doesn’t occur). -0.521
- I more often recall melodies in a minor, sad key than in a major, optimistic one. -0.509
- It often happens that I want to get sexually aroused, and the setting is right – but I just can’t, physically. -0.448
- I think my sexual needs and desires are weaker than those of my peers – I don’t really need it much now. -0.389
- I have problems with potency (reduced) (male). -0.434
- It’s true that neither erotica nor pornography really arouse me. -0.392
- I have acne on my face (or it appears periodically). -0.390
- I often experiment in sex, but not for enjoyment – just to stir up my weak sexual interest. -0.244
- I have some symptoms of osteoporosis (bone disease). -0.199
The questions in the scale show relatively weak profile consistency, but the result, despite lower profile contrast, is the same as with the single question about regularity of female menstruation. Namely, the psychotype with the highest average prolactin is ILI.
From the final socionic profiles in the presented table, one can also infer that high prolactin promotes increased Ni at the expense of both sensory functions, mainly Si; and declatim functions – at the expense of questim functions. From this, one can further assume (apparently not described in the scientific literature) that high prolactin levels suppress the activity of the insular cortex of the brain.